
A recent Black Book survey found that hospitals and other providers are gearing up to outsource key functions, including a move to outsource revenue cycle management to third-party vendors. Medical groups may well consider similar moves to maintain medical practice benchmarks.
The main reasons given by responders for outsourcing revenue cycle management were to reduce costs and prioritize value-based care reimbursement initiatives, which will be mandated this year.
Value-based care concentrates on patient outcomes rather than the number of medical office visits, hospitalizations, or referrals – quality over quantity. It calls for a multipronged but streamlined approach to achieve this goal and curb Medicare costs.
Value-based care reimbursement offers providers incentive payments when the quality of care over the quantity of care ideal is met or when adherence to value-based care is recognizable. This approach has prompted many providers to outsource revenue cycle management to third-party providers.
Value-Based Care Goals
The goals of value-based care reimbursement in relation to information provided by the Centers for Medicare and Medicaid Services include:
- Improved care for individuals.
- Maximizing Health IT.
- Improved health for populations.
- Decreased costs by paying for quality over quantity.
- Removing regulations that stand in the way of coordinated care.
The Department of Health and Human Services’ Centers for Medicaid & Medicare added to these goals with the release of the Fiscal Year 2019 Inpatient Prospective Payment System, which requires hospitals to:
- Post their prices on the internet and in a machine-readable format.
- Eliminate dated quality initiatives.
- Prompt providers to make their electronic health records interoperable.
Value-Based Care Realities
Despite all this coming down the pipe this year, a recent survey of 451 doctors and insurance executives conducted by Quest Diagnostics found that health care has made little progress toward the coming mandate to value-based care reimbursement since 2017 and may even have gone backward. Among those surveyed, more than 67% said they believe the U.S. has a fee-for-service system and not a value-based care system. This is an increase of almost 5% over the previous year’s findings.
Another survey by Deloitte in October of 2018 found that the healthcare industry is largely ill-equipped to deal with the coming changes, lacking both the tools and the data.
This survey mirrors previous findings from a joint value-based care study brought by Humana and the American Academy of Family Physicians. This survey found that less than 9% of family physicians believe that quality expectations are doable under value-based care models. Additionally, only 17% of physicians claimed to be extremely familiar with the concept of value-based care.
Yet, value-based care reimbursement mandates have arrived!
A Brief History of Value-Based Care
To understand what value-based care reimbursement will mean for your practice or hospital, you would do well to revisit the legislation or programs that came before – the phasing out of the fee-for-service model toward the implementation of value-based care reimbursement.
- 2008 – Medicare Improvements for Patients and Providers (MIPAA): The purpose of this legislation is to provide grants to states and tribes that assist individuals with disabilities, older persons, and their caregivers by applying for Medicare assistance.
- 2010 – Affordable Care Act (ACA): The purpose of this legislation is to bring affordable health care to more people.
- 2012 – End-Stage Renal Disease Quality Incentive Program (ESRD-QIP): The purpose of this program is to link part of reimbursement or claims to facilities that utilize quality care practices. This program also reduces payments to facilities when standards are not met. This is an early example of value-based care reimbursement.
- 2012 – Hospital Value-Based Purchasing (HVBP): Under this program, hospitals are reimbursed for the quality of care as opposed to the quantity. It’s another example of the progression toward value-based care reimbursement.
- 2012 Hospital Readmission Reduction Program (HRRP): Under this program, Medicare reduces reimbursements to hospitals with excessive readmissions following care.
- 2014 – Protecting Access to Medicare Act (PAMA): Under this legislation, providers utilizing advanced imaging must consult a qualified Clinical Decision Support Mechanism.
- 2014 – Hospital-Acquired Condition Reduction Program (HACRP): This program is a Medicare pay-for-performance incentive that links Medicare payments to inpatient hospital setting quality.
- 2015 – Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): This multi-part legislation considers the following: (1) various paths and multi-levels of risks and rewards for providers based on payments equating to value; (2) expansion for participation in alternative payment models; (3) scaling down reporting loads for alternative payment model involvement; (4) enhanced understanding of physician or provider status in respect to legislation; (5) support multi-payer initiatives.
- 2015 – Physician Value-Based Modifier (PVBM): This program measures the quality and cost of care for individuals with Medicare under the physician’s fee schedule.
- 2018 – Skilled Nursing Facility Value-Based Purchasing Program (SNFVBP): This program concentrates on better patient outcomes and rewards skilled nursing facilities with incentives for quality patient care and hospital readmission reductions.
The Argument for Value-Based Care Reimbursement
Value-based care reimbursement is set to replace the fee-for-service model across the board this year, which is why revenue cycle management outsourcing, as well as other kinds of outsourcing, may be surging.
Key strategies needed to thrive under the value-based revenue model include:
- Understanding the more unique requirements if you are part of an ACO, and APM or are affected by MIPS, to record the quality of care information for each model.
- Accurate data analytics produced by intuitive software and experts.
- Maximizing claims following accurate data analytics.
- Freeing up staff, including medical professionals, to see more patients and further increase revenue.
- Improved claims tracking.
- Improved patient outcomes through coordinated care.
- Streamlined medicine that allows providers to treat more patients.
- Revenue goals met and exceeded through optimized patient care and increased time management.
Taking measures to comply with value-based care reimbursement sounds simple. However, when you consider that only 17% of physicians surveyed claimed familiarity with the concept, it is apparent that something is lost in translation or the language is simply too vague or too robust.
Value-Based Care Requirements for Reimbursement
The Merit-Based Incentive Payment System (MIPS) began in 2017. Compensation under this value based care reimbursement model will be made this year.
Reimbursement is based on scores up to 100, and the MIPS model currently considers four categories: (1) Quality (50%); (2) Advancing care information (promoting interoperability) (25%); (3) Improvement activities (15%); and (4) Cost (10%).
Reimbursement or payment adjustment this year, based on your practice group’s 2017 MIPS score, works like this: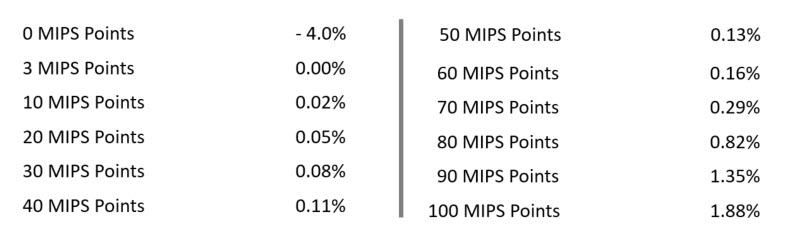 Value-based reimbursement changes for this year – the reimbursement year – include a MIPS overhaul:
Value-based reimbursement changes for this year – the reimbursement year – include a MIPS overhaul:
- Various healthcare professionals will be eligible and affected by MIPS, including rehabilitation therapists and other providers.
- MIPS exclusions will include professionals enrolled in Medicare Part B for the first year, practices with Medicare billed charges of less than $90,000 annually or less than 200 Part B patients, and clinicians taking part in other advanced payment models that collect one-quarter of Medicare reimbursements from these models.
Penalties for nonparticipation in MIPS and advanced payment models will increase by 5% for 2018 performance and continue increasing 2% per year over the next two years, which adds up quickly! The Alternative Payment Model (APM) is a substitute for MIPS, and this year, providers will have to choose between the two value-based care reimbursement models.
APM is an incentive and risk model that calls for providing high-quality and cost-effective care. An APM can mean providing care for specific conditions, episodes, or demographics. A risk and reward arrangement is created between health providers and payers – for example, the Medicare Shared Savings Program or an Accountable Care Organization. When a provider makes the decision to join an APM entity, that provider is motivated by financial incentives, in theory, to provide quality and cost-effective patient care.
The disparity between MIPS and APMs is that the latter comes with greater financial risks and greater potential for profit.
What Is Coming Up This Year
The move away from fee-for-service to value-based care reimbursement has been in the talking phase prior to the 2008 timeline. In fact, the introduction to value-based care reimbursement has been two decades in the making. Moreover, hospitals have been outsourcing revenue cycle management since 2016, based on the coming value-based care model, according to IT News.
According to an article published in Recycle Intelligence, value-based care counts on clinical data to score compliance. Starting this year, using revenue cycle analytics to optimize and enhance your practice group’s MIPS score is a must.
It may be time to consider an operational review focused on revenue cycle management and this year’s Value Based Care models, including your preparedness for the implementation of MIPS.
2019 is here, what are you waiting for?